




Zepbound® vs Mounjaro® for Weight Loss: A Simple Guide


Zepbound® vs Mounjaro® for weight loss: both contain tirzepatide, but they’re FDA-approved for different uses. See weight-loss results reported in studies by dose, common side effects, and how to think about on-label vs off-label use. Individual results vary.
When it comes to choosing between Zepbound® vs Mounjaro® for weight loss, one thing to remember: they both contain tirzepatide. So at the same dose, results are expected to be similar (individual results vary). The biggest difference is what the FDA officially says each drug is for (weight management vs. type 2 diabetes), and how that affects who is eligible and how it’s covered by insurance.
- Study results: Higher doses were linked with greater average weight loss in studies, but real-life results vary.
- Side effects: GI symptoms are most common (nausea, diarrhea, constipation, vomiting), especially during dose increases.
- What matters most: Your health history, goals, and what you can tolerate or access usually matter more than the name on the box.
*Study note: The obesity weight loss data commonly cited comes from tirzepatide, later marketed as Zepbound®; diabetes comparative trials used tirzepatide marketed as Mounjaro®.
Disclaimer: Educational content and not medical advice. Discuss any medication with your licensed healthcare provider. For FDA-approved drugs, see each manufacturer’s full prescribing information.
Weight loss results: Zepbound® vs Mounjaro®
In the FDA labeling for Zepbound® (tirzepatide), weight loss at 72 weeks was dose-dependent in adults without type 2 diabetes:
5 mg: ~15.0% average weight loss
10 mg: ~19.5% average weight loss
15 mg: ~20.9% average weight loss
In adults with type 2 diabetes (also 72 weeks), average weight loss was typically lower:
10 mg: ~12.8% average weight loss
15 mg: ~14.7% average weight loss
These are study averages and aren’t a guarantee of individual results.
Why was there a difference? People with type 2 diabetes often lose less weight on average than people without diabetes, and these studies were designed for different goals. So it’s easy to draw the wrong conclusion if you compare headline results without looking at who was in the study.
Is Zepbound® “Better” for Weight Loss Than Mounjaro®?
If someone takes tirzepatide at the same dose regardless of the medication name, the medication effect should be similar. What people really mean by “better” usually comes down to:
- On-label vs off-label: Zepbound® is FDA-labeled for weight management; Mounjaro® is labeled for type 2 diabetes. As of Dec 20, 2024, Zepbound® is also FDA-approved for moderate-to-severe OSA in certain adults with obesity.
- Study population differences: obesity trials (no diabetes) often show higher average weight loss than diabetes trials.
- Coverage differences: insurance often follows labeled indication, which can drive what people can access.
What this really means–It’s not that the ingredient “works better” in one brand. It’s that Zepbound® is studied/labeled for weight management, so that’s how it’s discussed, prescribed, and covered, which tends to align more directly with weight-loss goals.
{{primary-cta}}
Dosing
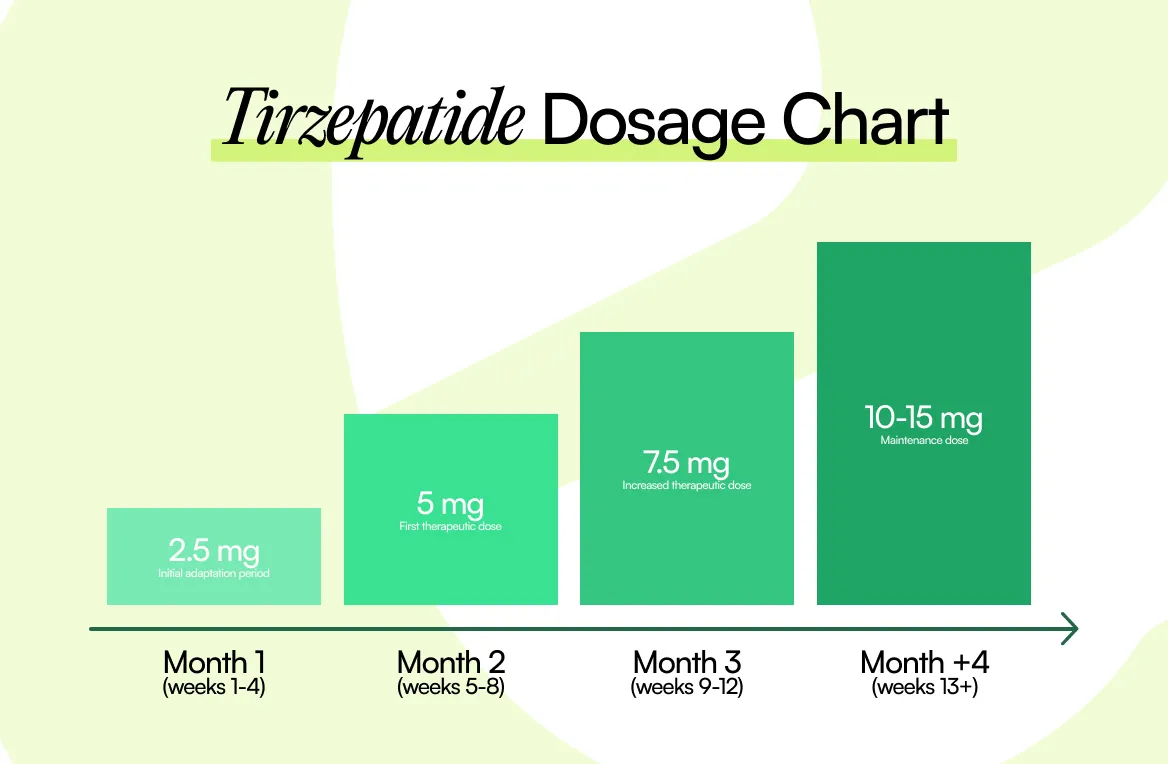
Dosing and titration schedules are similar across tirzepatide products: people typically start at a low dose and increase gradually over time. In the Zepbound® weight-management trials, doses were titrated up to maintenance doses (e.g., 5, 10, or 15 mg), with weight assessed at 72 weeks. Keep in mind that only your prescriber can determine your dosing plan.
Side Effects (What People Notice First)
Because the active ingredient is the same, the most common side effects overlap. GI effects are the ones most people ask about—nausea, vomiting, diarrhea, constipation, abdominal discomfort—often appearing during dose increases and improving for many people over time (not guaranteed).
Both medications have important warnings and potential serious risks (including the boxed warning). Review the full prescribing information and talk with your clinician about what applies to you.
How to Decide Which is a “Better” Fit
Zepbound® may be a better fit if:
- Your goal is chronic weight management, and you want an option labeled for that use, and/or
- You and your clinician are navigating coverage where label indication matters.
Mounjaro® may make more sense if:
- You have type 2 diabetes, and weight loss is a meaningful secondary goal alongside glycemic control.
The practical reality:
A lot of the time, people discuss both options because insurance coverage and access end up determining what’s realistic.
{{primary-cta}}
Cost & Coverage
For most people, the “real-world” difference comes down to what your plan will cover.
- Coverage varies a lot and often depends on the FDA-labeled use (weight management vs type 2 diabetes).
- Without coverage, costs can be high: reported list prices are often >$1,000/month, but what you actually pay depends on your plan, pharmacy pricing, and eligibility for manufacturer programs.
- You may need prior authorization at times: plans may require documentation (diagnosis/BMI criteria, prior attempts, etc.), and requirements vary by insurer.
Tip: If you’re unsure what your plan covers, ask your insurer whether tirzepatide is covered under your plan for weight management vs type 2 diabetes, and what documentation is needed.
Conclusion
Zepbound® and Mounjaro® use the same medication (tirzepatide), so the most important differences for weight loss usually come down to FDA-labeled use, how the study results apply to you, and what your coverage allows. If you’d like support sorting through it all, Eden can help you set up a conversation with a licensed clinician to talk through options and a plan that fits your goals.
Eden is an independent company and is not affiliated with, sponsored by, or endorsed by Eli Lilly and Company; all trademarks are the property of their respective owners. Names are used for identification and educational purposes only.







The FDA does not approve compounded medications for safety, quality, or manufacturing. Prescriptions and a medical evaluation are required for certain products. The information provided on this blog is for general informational purposes only. It is not intended as a substitute for professional advice from a qualified healthcare professional and should not be relied upon as personal health advice. The information contained in this blog is not meant to diagnose, treat, cure, or prevent any disease. Readers are advised to consult with a qualified healthcare professional for any medical concerns, including side effects. Use of this blog's information is at your own risk. The blog owner is not responsible for any adverse effects or consequences resulting from the use of any suggestions or information provided in this blog.
Eden is not a medical provider. Eden connects individuals with independent licensed healthcare providers who independently evaluate each patient to determine whether a prescription treatment program is appropriate. All prescriptions are written at the sole discretion of the licensed provider. Medications are filled by state-licensed pharmacies. Please consult a licensed healthcare provider before making any medical decisions.
Frequently asked questions
Is Zepbound the same as Mounjaro for weight loss?

They contain the same active ingredient (tirzepatide), so at the same dose, they’re expected to have similar medication effects. Differences in reported results often reflect different trial populations and indications.
Why do Zepbound trials show higher average weight loss than diabetes trials?
Obesity trials often enroll people without diabetes and measure weight as the primary endpoint; diabetes trials enroll people with type 2 diabetes and focus on glucose control, and average weight loss is often lower.
Which one has fewer side effects?
Side effects are similar because the ingredient is the same. GI effects are common, and both have important warnings; your clinician can help weigh risks based on your history.
Can someone use Mounjaro® for weight loss?
Off-label use is something you’d talk through with a licensed prescriber, who can help decide whether it’s appropriate for your situation.
Who should avoid tirzepatide medicines?
People with certain contraindications (including personal/family history of medullary thyroid carcinoma or MEN2) and other risk factors should not use these medications; review the full prescribing information with a clinician.
Related articles








Aetna. (2024). Zepbound prior authorization with limit policy (6192-C). https://www.aetna.com/products/rxnonmedicare/data/2024/Zepbound_PA_with_Limit_6192-C_P08-2024_R.html
Centers for Disease Control and Prevention, National Center for Health Statistics. (2024). Obesity and severe obesity prevalence in adults: United States, August 2021–August 2023 (NCHS Data Brief No. 508). https://www.cdc.gov/nchs/products/databriefs/db508.htm
Dahl, D., Onishi, Y., Norwood, P., Huh, R., Bray, R., Patel, H., & Rodríguez, Á. (2022). Effect of subcutaneous tirzepatide vs placebo added to titrated insulin glargine on glycemic control in patients with type 2 diabetes: The SURPASS-5 randomized clinical trial. JAMA, 327(6), 534–545. https://doi.org/10.1001/jama.2022.0078
Eli Lilly and Company. (2022). MOUNJARO (tirzepatide) injection, for subcutaneous use: Prescribing information. U.S. Food and Drug Administration. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215866s000lbl.pdf
Eli Lilly and Company. (2024). ZEPBOUND (tirzepatide) injection, for subcutaneous use: Prescribing information. U.S. Food and Drug Administration. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/217806s003lbl.pdf
Frías, J. P., Davies, M. J., Rosenstock, J., Pérez Manghi, F. C., Fernández Landó, L., Bergman, B. K., Liu, B., & Fernández, L. (2021). Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. The New England Journal of Medicine, 385(6), 503–515. https://doi.org/10.1056/NEJMoa2107519
Gasoyan, H., et al. (2025). Changes in weight and glycemic control following obesity pharmacotherapy with semaglutide or tirzepatide in real-world practice. Obesity. https://doi.org/10.1002/oby.24331
Jastreboff, A. M., Aronne, L. J., Ahmad, N. N., Wharton, S., Connery, L., Alves, B., Kiyosue, A., Zhang, S., Liu, B., Bunck, M. C., & Stefanski, A. (2022). Tirzepatide once weekly for the treatment of obesity. The New England Journal of Medicine, 387(3), 205–216. https://doi.org/10.1056/NEJMoa2206038
Office of the Assistant Secretary for Planning and Evaluation (ASPE). (2024). Medicare coverage of anti-obesity medications (Issue Brief). U.S. Department of Health & Human Services. https://aspe.hhs.gov/sites/default/files/documents/127bd5b3347b34be31ac5c6b5ed30e6a/medicare-coverage-anti-obesity-meds.pdf
Office of the Commissioner. (2024, December 20). FDA approves first medication for obstructive sleep apnea. U.S. Food And Drug Administration. https://www.fda.gov/news-events/press-announcements/fda-approves-first-medication-obstructive-sleep-apnea
U.S. Congressional Research Service. (2024). Medicare coverage of GLP-1 drugs (In Focus IF12758). https://www.congress.gov/crs-product/IF12758
Eli Lilly and Company. (2025). Zepbound prior authorization resource guide (payer reference). https://zepbound.lilly.com/assets/pdf/zepbound_Prior_Authorization_Resource_Guide.pdf
Thank you!
We'll be in touch.
Thank you!

